Inflammation Mastery, 4th Edition = 1200 pages + 30h video: Efficient and Effective Treatment of a Wide Range of Common Diseases based on DrV's Functional Inflammology Protocol (video) and Expert-level medical-clinical integration (video).
Now available from: BookDepository.com: free delivery worldwide; Amazon.com: paper and digital ebooks; Barnes and Noble.com: best prices paper/digital; ThriftBooks; AbeBooks; BetterWorldBooks; WaterStonesBooks
Bulk discounts are still available for student groups / required textbook shipped to the same address; contact admin@ichnfm.org for details and qualifications
See DrV's new Newsletter, Videos, Courses, and Blog: https://healthythinking.substack.com/p/selfpaced-learning-antiviral-nutrition

Translating Microbiome (Microbiota) and Dysbiosis Research into Clinical Practice: The 20-Year Development of a Structured Approach that Gives Actionable Form to Intellectual Concepts
Alex Vasquez DC ND DO FACN, ICHNFM

A 39-minute introductory video (relevant for the PDF article): Many video samples are available from our ICHNFM website; see Functional Inflammology, part 1, CME course introduction, gut-brain axis, fibromyalgia, and many other videos.
Download PDF for articles, images, and video links
Introduction, Perspective, Context
Many years ago when I published my first books[1,2] and articles[3] detailing "dysbiosis", the word could hardly be found in the Medline index, the topic was controversial at best and ethereal at worst, the term "microbiome" (first published in French in 1949 and in English in 1988) was virtually unknown, and I spent most of the time and space in my lectures and articles substantiating and defending the condition's existence. These days, everyone is talking about microbiome, dysbiosis, "leaky gut" (thanks largely to Leo Galland MD), and my 1996 article on “Silent Infections and Gastrointestinal Dysbiosis" has been downloaded at least 6,500 times and is one of the top 1% most popular articles on Academia.edu.[4] In the preparation of my dysbiosis lecture at a major functional medicine conference in 2010, I found that only 180 Medline articles indexed the term “dysbiosis”, and now—slightly less than five years later—more than 1,200 articles index that term. Obviously, the dysbiosis concept has become better known to the point of actually being popular, but this does not mean that clinicians understand what to do with it. A recent article from the June 2015 issue of Nature Medicine perfectly summarized this discrepancy between microbiota research and clinical action: "In the three years since the completion of the first phase of the Human Microbiome Project, the number of scientific papers linking the microbes that live in our gut to diseases ranging from diabetes and colitis to anxiety and depression has grown exponentially. Yet, these tantalizing connections have yielded few benefits from a therapeutics standpoint."[5] To the extent that this information is being integrated into clinical practice at all, the current level of practical application is a bit indelicate and cumbersome beyond the most commonly repeated advice of advocating probiotics, avoiding antibiotics, perhaps delving into using botanical antimicrobials and laboratory testing. Breath testing (an insensitive test for only one subtype of gastrointestinal dysbiosis) and microbiologic testing have become popular to the point of overuse as doctors grapple for clinical clues. (Noteworthy in the conversation on functional laboratory testing is that one functional medicine laboratory in particular used inaccurate proprietary microbe-identification methods to extract millions of dollars of patient and physician money only to deliver innumerable wasted hours in patient suffering and physician confusion due to misleading and worthless [e.g., "parasite present: taxonomy unavailable"] laboratory information.[6]) So, despite the bloom in research and the exponential public awareness of dysbiosis, much progress still needs to be made in order to help clinicians—and ultimately patients—better appreciate, assess, optimize and maintain microbiotal health—eubiosis.
"Dysbiosis is an important concept, but doctors cannot treat concepts. We have to define, describe, and deconstruct the microbes, molecules, and mechanisms into their components, then rebuild a conceptual scaffold and intellectual structure that becomes a useful tool that, with study and experience, can be used in a clinical setting to effective benefit." Alex Vasquez DC ND DO FACN
Clinical Importance
The priority is to understand the role of dysbiosis in clinical disease; patients are suffering day-by-day and hour-by-hour because of microbial colonization, bacterial allergy, reactive arthritis, systemic inflammation, fibromyalgia, insulin resistance, neurocognitive impairments, autoimmunity, and other manifestations of dysbiosis. The basic science and clinical research data on these various phenomena is crystal clear and intellectually sound but is rarely delivered in a manageable manner so that time-pressured clinicians can perceive the information in an interconnected context that expedites clinical application in patient assessment and treatment. Personally, I have generally approached clinical care with a sense of urgency, for altruistic reasons and because I know the experience of being persistently ill—in my case, the situation lasted for seven years and still occasionally recurs, as discussed later.
Dysbiosis-Triggered Illness: Deconstructing the Phenomena and Helping Our Patients
Dysbiotic illness can ultimately be understood as a manifestation of human intolerance of the total microbial load (TML) and more specifically the total dysbiotic load (TDL) which is only one part of the total inflammatory load (TIL), alternately described as the total impairment load—that is, the total load of physiologic, biochemical, and psychosocial burdens that promote inflammation or any type of metabolic/physiologic/mental impairment. As I have said for many years, dysbiosis is a disease state best described as a "bad relationship" wherein neither the host nor the microbe(s) are unilaterally "at fault" but rather that they are—for a variety of modifiable and nonmodifiable reasons—currently incompatible. Conceptualizing dysbiotic illnesses as a relationship rather than as an infection—an extension of the acute infection model wherein the microbe is presumed guilty gives us three major areas of intervention: immunorestoration, tolerogenic or adaptive, antimicrobial.
Personal Experience
I did not become an expert in dysbiosis entirely by choice; I had to become so in order to literally save my own life and preserve my own health. The year was 1995, the idea of "leaky gut" was new and ridiculed (in contrast to its wide acceptance today), and the entire concept of functional medicine had only been announced just a few years prior. Thanks to mostly to Metchnikoff, the naturopathic profession, a handful of allopathic doctors, and a few scattered and vintage medical articles, we had some vague ideas about dysbiosis but very few details with which to understand it better, let alone treat it effectively. In this case, I am discussing gastrointestinal dysbiosis, which is the prototype but obviously only one of the eight location-based subtypes of dysbiosis.
I remember the exact day and moment that it all started. What began with the typical "brain fog" later progressed to physical inertia, multiple chemical sensitivity / environmental intolerance (MCS/EI), and progressive immediate-onset food allergies, most of which were frustratingly unidentified except for soy lecithin—of note, 1996 was the first year of genetically manipulated (GM) soy in the US. I was also progressively lymphopenic and had remarkable responses to parenteral vitamins, especially vitamin B12 (improved mental clarity) and folic acid (resolution of progressive lymphopenia). See PDF for laboratory results. At this time, I was finishing chiropractic college, starting naturopathic college, and harvesting gems from every seminar, book, and audiocassette I could find, notably from Bland, Galland, Gaby and Wright. With new access to the internet, I scoured the earlier versions of Medline and spent my evenings and weekends in the medical libraries at Oregon Health Science University in Portland and University of Washington in Seattle. I started compiling and publishing articles, and my main research interests at the time—other than studying everything nutrition and trying to find solutions to my own mysterious illnesses—were rheumatology and hemochromatosis.[7]
Following graduation and licensure, I opened a clinical practice in Seattle, and later I was also invited to teach Orthopedics and Rheumatology at Bastyr University. The responsibility of teaching these courses gave me reason to dive even deeper into the research and to begin articulating and giving structure to what almost always starts as inklings and impressions. Slowly, I started to understand dysbiosis, its various permutations, and the variances of effect that different microbes could have, either in isolation or in combination—what I would later elucidate as combinatorial dysbiosis[8] and continue to refine on an almost daily and regular basis.[9]
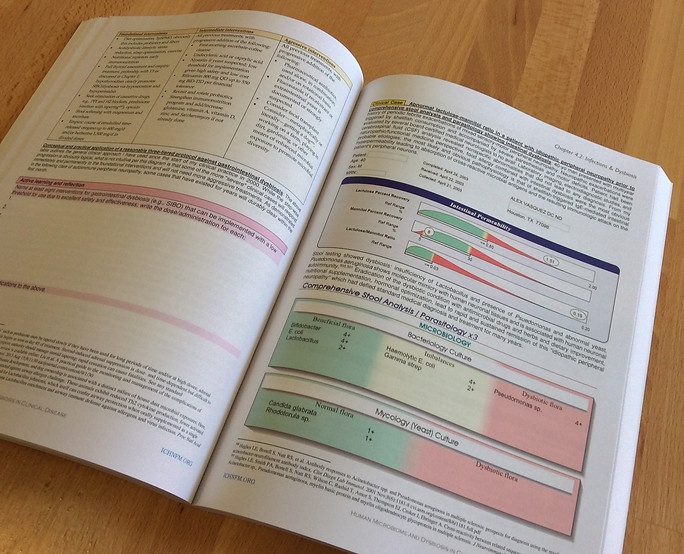
With effort and reflection, obscurity morphed into clarity. If all we had to work with is the laboratory result above, this alone would have been sufficient to explain and solve all my health problems within hours; I have this level of understanding now, but only after studying the topic—not simply for academic reasons or in a cursory manner, but with some sense of personal urgency—for twenty years. The main findings of the results above are the Citrobacter freundii and the Klebsiella pneumoniae, and additional finding on this same result was that of markedly elevated fecal beta-glucuronidase. With years of trial and error and a high degree of certainty based on personal experience backed by a massive review of the research literature, I would interpret the above results as follows:
-
The mental and physical fatigue I experienced were due mostly to hydrogen sulfide (H2S) produced by the Citrobacter freundii. H2S is a mitochondrial toxin and thus a neurotoxin, thereby explaining the fatigue, and it also chelates cobalamin, thereby explaining the response to vitamin B12, indicative of vitamin B12 deficiency, which was also contributing to the fatigue. Constipation was another problem that was not only miserable, but which also promoted the persistence of the dysbiosis and which was caused by the gut-paralyzing effect of H2S.
-
The multiple chemical sensitivity / environmental intolerance (MCS/EI) was due to impaired cytochrome p450 detoxification secondary to endotoxin in general and the O antigen of Klebsiella pneumoniae in particular. Additively and synergistically, the elevated fecal beta-glucuronidase was deconjugating whatever little cytochrome p450 detoxification was taking place, leading to the inability to clear and thus the accumulation of ambient chemicals and internal toxins that could not be oxidized for conjugation; notice the dual effect of endotoxin-mediated blockade of cytochrome p450 along with increased enterohepatic recycling due to the elevated fecal beta-glucuronidase. The folate deficiency and resultant lymphopenia are presumed due to a combination of malabsorption and increased utilization; at this time I also had an increased lactulose:mannitol ratio and dramatically elevated caffeine clearance with horrid benzoate conjugation.
-
Immediate-onset food allergies were due to the increased intestinal permeability and immune activation, both of which can be blamed on elevated gastrointestinal endotoxin.
During this time, I gained personal physician heal thyself experience with practically innumerable nutrients, botanicals, and a few antimicrobial drugs; I also appreciated—and was ultimately cured by—my (in)famous vitamin C purge: first-morning consumption of two cups of coffee (peristalsis stimulant) and ~30 grams of vitamin C with the resulting osmotic laxative and exaggerated migratory motor complex providing gastrointestinal housecleaning par excellence.
Conclusions
With the compilation of personal experiences and ongoing research from thousands of clinicians and basic scientists, we collectively have the knowledge and tools available to assess and alleviate dysbiotic illnesses in their various forms. The twilight of the idiopathic era and the dawn of new possibilities in health and healthcare continue to be progressively illuminated.[10]






FOR CLARITY: Chapter 5.1b from Inflammation Mastery 4th Edition was published separately as
Pain Revolution in color and later as
Brain Inflammation in discounted grayscale; the digital versions are identical.


The text of "Neuroinflammation in fibromyalgia and CRPS is multifactorial" published in Nature Reviews Rheumatology (March 2016) is included in the printed versions of Inflammation Mastery 4th Edition, Pain Revolution and Brain Inflammation.


Support this work that benefits you. To bring you this work, our costs include websites, software, video hosting, press releases, massive amounts of faculty time for research, presentation, editing, curation, professional fees, certifications and accreditations...
1. Enjoy the work: Free journal articles, excerpts, social media updates, and blogs with clinical importance, low-cost ebooks for managing migraine, fibromyalgia, viral infections, mTOR, press releases
2. Benefit from the work: Enhance your practice and clinical success with masterpiece books and courses that do more than pay for themselves, excellent ROI (return on investment)
3. Support the work: Purchase an online course, ebook, monograph, textbook or donate via GoFundMe.









[1]. Vasquez A. Integrative Rheumatology. Integrative and Biological Medicine Research and Consulting, 2006. * Now updated as Inflammation Mastery.
[2]. Vasquez A. Musculoskeletal Pain: Expanded Clinical Strategies. Institute for Functional Medicine, 2008. * Now updated as Inflammation Mastery..
[3]. Vasquez A. Multifocal dysbiosis: Pathophysiology, relevance for inflammatory and autoimmune diseases, and treatment with nutritional and botanical interventions. Naturopathy Digest 2006 Jun http://www.ichnfm.org/faculty/vasquez/reprints/2006_multifocal_dysbiosis.html
[4]. Vasquez A. Nutritional and Botanical Treatments Against “Silent Infections” and Gastrointestinal Dysbiosis, Commonly Overlooked Causes of Neuromusculoskeletal Inflammation and Chronic Health Problems. Nutritional Perspectives 2006 Jan. http://ow.ly/O0Wau
[5]. de Vrieze J. Microbiome models, on computers and in lab dishes, see progress. Nature Medicine 2015 June; 21: 543–544 www.nature.com/articles/nm0615-543
[6]. Gingras BA, Duncan SB, Scheuller NJ, Schreckenberger PC. Assessment of diagnostic accuracy of recently introduced DNA stool screening test. International Journal of Human Nutrition and Functional Medicine 2014;v2(q1);p1 http://ow.ly/O2eRE
[7]. Vasquez A. Musculoskeletal disorders and iron overload disease: comment on the American College of Rheumatology guidelines for the initial evaluation of the adult patient with acute musculoskeletal symptoms. Arthritis Rheum. 1996 Oct;39(10):1767-8 http://www.ncbi.nlm.nih.gov/pubmed/8843875
[8]. Vasquez A. Now updated as Inflammation Mastery.
[9]. Vasquez A. Human Microbiome and Dysbiosis in Clinical Disease. International College of Human Nutrition and Functional Medicine, 2015. [ISBN 1512360295 / 9781512360295] https://www.createspace.com/5518130
[10]. Vasquez A. Idiopathic versus Multifactorial: Twilight of the Idiopathic Era and the Dawn of New Possibilities in Health and Healthcare. Naturopathy Digest 2006